脑损伤
-
Figure 1|Flow diagram of the process of selecting studies for review.

Since the 1960s, axonal injuries have been reported in patients with concussion (mTBI) through autopsy studies conducted after the patients died from other diseases without any lesions observed on conventional brain computed tomography or MRI. Organic brain injuries have also been demonstrated by a variety of other tests, such as the nuclear medicine and neurophysiologic tests and electroencephalography (Blumbergs et al., 1994; Major et al., 2015; Bonfante et al., 2018; Raji and Henderson, 2018). With respect to DTI, cerebral white matter injury and axonal injury in concussion (mTBI) have been reported in hundreds of articles published in international journals since 2002, and dozens of studies have demonstrated axon injuries in concussion (mTBI) patients by applying DTT (Shenton et al., 2012; Yallampalli et al., 2013; D’Souza et al., 2015; Kim et al., 2015a; Lee and Jang, 2015; Jang and Kim, 2016; Jang and Lee, 2017a, b; Jang, 2018). In the above studies, two DTI-based analytical methods have been used to detect axonal injury in concussion (mTBI): 1) measurement of DTI parameters such as fractional anisotropy and mean diffusivity in specific regions of interest of the brain, and 2) DTT assessment of neural tracts, assessment of DTT parameters such as fractional anisotropy, mean diffusivity, and tract volume, and configurational analysis of reconstructed tracts (Jang, 2018). The main advantage of DTT over DTI is that it allows the entire neural tract to be evaluated based on a variety of DTT parameter measurements. In addition, configurational analysis of reconstructed neural tracts can indicate abnormalities such as tearing, narrowing, or discontinuations, which have been used to identify axonal injury of neural tracts in concussion (mTBI) patients (Jang, 2018). Although many of the characteristics of axonal injury in concussion (mTBI) observed on DTT have not yet been fully elucidated, and much research is still needed, several characteristic features have been reported. In this review, we selected relevant studies according to the process presented in the flow diagram in Figure 1.
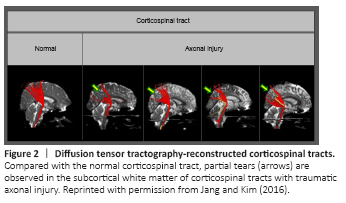
Figure 2|Diffusion tensor tractography-reconstructed corticospinal tracts.
In this review, DTI studies that have demonstrated characteristics of axonal injury in concussion and mild traumatic brain injury are reviewed. Relevant studies published during 2009 to 2020 were identified by searching the following electronic databases: PubMed, Google Scholar, and MEDLINE. The following key words and abbreviations were used to search the databases: DTI, DTT, mTBI, concussion, axonal injury. This review was limited to studies of humans. We selected relevant studies according to the flow diagram shown in Figure 2.
Figure 3| Results of brain magnetic resonance imaging and diffusion tensor tractography in patients injured by a motor vehicle accident.

In concussion (mTBI) patients, it has been reported that neural structures show more damage in the anterior portion than in the posterior part (Cubon et al., 2018). Regarding the cingulum, Jang et al. (2013) conducted a study of the injury of the cingulum in 21 diffuse axonal injury patients with cognitive impairment and reported that the most severe nerve damage occurred in the anterior cingulum located in the frontal lobe. Likewise, the major common injury feature appearing in other case reports was discontinuation in the anterior portion of the cingulum in concussion (mTBI) patients (Figure 3) (Kim et al., 2015a). Damage to the arcuate fasciculus of the dominant hemisphere was observed in 39% of patients, with the identified characteristic damage patterns being narrowing and discontinuation, and all of the cases of discontinuation involved injury of the anterior portion of the arcuate fasciculus that is connected to Broca’s area.
Figure 4| Results of diffusion tensor tractography of the fornix (right – red, left – yellow) of patients with mild traumatic brain injury.
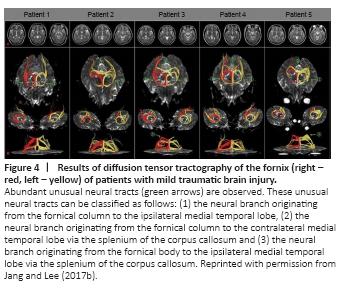
Figure 5| Mechanisms of recovery of injured fornical crus as determined by diffusion tensor tractography.

A previous study of the fornix in diffuse axonal injury has reported that the fornix injury pattern is characterized by discontinuation of the fornical crus (Jang et al., 2009a). In mTBI cases, Jang and Lee (2017b) reported that discontinuation of the fornical crus or fornical column was observed in 86 patients with memory loss following mTBI, and an additional distinctive injury pattern observed only in the fornix was the formation of collateral branches of the fornix following injury (Figure 4). These collateral branches form a recovery or compensation mechanism following fornix injury, providing a connection to the medial temporal lobe, which is the normal fornix pathway, by extending nerve branches along various pathways from the damaged fornical crus, fornical body, and fornical column (Figure 5). In TBI, the impact on the brain might be relatively weaker than that in diffuse axonal injury, and it is suggested that, while the partially damaged fornix is recovering, collateral branches going toward the ipsi-lesional medial temporal lobe or contra-lesional medial temporal lobe may be formed (Jang and Lee, 2017a).